Pediatrics & Neonatology - Juniper Publishers
Objectives: This study aims at evaluating whether muscle training using moderate loads will cause an increase in inspiratory muscle strength, which was assessed by the measurement of maximal inspiratory pressure (PIMAX) in patients dependent on mechanical ventilation.
Methods: This is a retrospective study conducted in 2 Pediatric Intensive Care Units from January 2016 to December 2017. All patients who underwent muscle training during the period of the study were included. PIMAX was measured using a manovacuometer. Three measurements were made with an occlusion time of 15 seconds and a recovery interval of 2 minutes between them. Muscle training was performed following the institutional protocol (4 sets of 6 repetitions with a load equivalent to 60% of PIMAX) 1x/day, 6 days a week, excluding the day of the measurement of PIMAX.
Results: Six patients undergoing prolonged mechanical ventilation (average time of mechanical ventilation of 9647 hours) who underwent muscle training to disconnect mechanical ventilation were included. The measurements of PIMAX pre-training were compared to weeks 1 to 4. A significant difference on PIMAX was observed after the second week of training (p <0.001). Five patients progressed to IMV disconnection.
Conclusion: Our study supports the performance of IMT using moderate loads (60%), without risk of muscle fatigue as it resulted in a significant increase in PIMAX after 2 weeks of training, with positive outcomes regarding weaning from mechanical ventilation.
Keywords: Inspiratory muscle training, pediatrics, muscle strength, maximal respiratory pressure
Introduction
For patients under invasive mechanical ventilation (IMV), about 30% of patients evolve to prolonged weaning, and 5% has been dependence on IMV. When weaning failure occurs, the assessment of causes must be guided by three pillars: inadequate respiratory drive, increased respiratory effort, and weakness of the respiratory muscles [1]. For decades, ventilator-induced diaphragmatic dysfunction has been described as one of the main complications of IMV and it involves structural myofibrillar lesions leading to atrophy and functional abnormality [2-4]. Diaphragmatic weakness has been associated with an imbalance between myofibrillar protein synthesis and muscle proteolysis [5]. Furthermore, in critically ill patients, immobility, systemic infection, and inflammation may contribute to skeletal muscle dysfunction [6,7].
Inspiratory muscle training (IMT) with a linear load device has been performed in adult patients with good outcomes. It was observed increased inspiratory muscle strength, increased inspiratory muscle resistance, dyspnea reduction, increased exercise tolerance and improved quality of life [8]. Initially, the loads used were extremely low (20-30% of PIMAX) as it was feared high loads would cause muscle fatigue. However, this training profile had no impact on PIMAX or on outcomes of disconnection from IMV [9,10]. The training of adults with moderate to high loads was described by Martin et al as having excellent results in terms of disconnection from the IMV, with no report of muscle fatigue and significant increase in PIMAX [11,12].
There is still a scarcity of literature on pediatric population, and most of it consists of descriptions of isolated case reports evaluating low-load muscle training in patients with difficult ventilator weaning [13,14].
Objectives
This study aims at assessing whether moderate-load muscular training increases the inspiratory muscle strength, which was evaluated by measurements of maximal inspiratory pressure (PIMAX) in patients dependent on mechanical ventilation.
Methods
This is a retrospective study conducted in 2 Pediatric Intensive Care Units from January 2016 to December 2017. All patients who underwent muscle training during the period of the study were included. This research involving human participants all clinical investigation were conducted according to the principles expressed in the Declaration of Helsinki (1975, revised in 2000) and that it meets the ethical guidelines, including adherence to the legal requirements of the study country. The research was submitted to the ethics committee: Ethics and research committee of the Albert Einstein Hospital number: 62561516.9.2001.0071 and Ethics and research committee of Municipal Health Secretary number: 62561516.9.0000.0086. The informed consent term was waived by the ethics and research committee. This study received no funding.
The study included patients who underwent muscle training and were admitted to the Pediatric Intensive Care Units of two hospitals – one private and the other public – in the city of São Paulo, from January 2016 to December 2017.
Measurement of maximal inspiratory pressure
For the PIMAX measurements we used a Murenas manovacuometer (Juiz de Fora, MG, Brazil) with a scale from 0 to 150 cm H2O and variations of 5 cm H2O. Three measurements were made, with an occlusion time of 15 seconds and a 2-minute interval between them. During the interval, the patient was reconnected to the mechanical ventilator for recovery. Ventilation was measured using the pre-established protocol by trained physiotherapists.
Muscle training
Low intensity muscle training is defined when loads below 50% are used, moderate intensity muscle training when the loads used range from 60 to 80%, and high intensity muscle training when loads are greater than 90%. The higher the load, the lower the number of repetitions must be used. The training followed an institutional protocol of 1x/day, 6 days a week, excluding the day of the measurement of PIMAX. The training consisted of 4 sets of 6 repetitions for each section with a load calculated at 60% of PIMAX. The device used for muscle training was Threshold IMT (Respironics Inc; Murrysville, PA, USA).
Statistical Analysis
Regarding quantitative variables, the sample was characterized by mean, standard deviation, minimum and maximum, median and percentages; regarding qualitative variables, the sample was characterized by relative and absolute frequencies. To assess patients’ strength gain, we used the Generalized Estimation Equation Model – GEE. The dependent variable was PIMAX, and the independent variables were time (in weeks) and age (in months). Residual analysis was performed graphically. The analyses were performed using SPSS software (IBM Corp, 2016), v23.0, and a significance level of 5% was considered.
Results
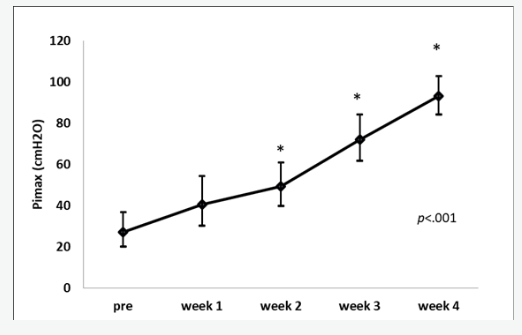
Six patients in prolonged mechanical ventilation and undergoing muscle training in to be disconnected from mechanical ventilation were included. Table 1 presents the main demographic characteristics and post-training outcomes. Table 2 shows the estimated averages in a model that considered age as a control covariate given the variability of patients age. It also includes comparisons between the different stages with Bonferroni correction of the p-value. Pre-training PIMAX was compared to the PIMAX on weeks 1 to 4; only two patients showed results at week 4. We observed a significant difference in PIMAX after the second week of training. Figure 1 shows the patients’ average PIMAX profiles over time. We can observe a significant increase in PIMAX from the second week on.
Discussion
Our study was the first to conduct moderate load (60% of PIMAX) inspiratory muscle training in pediatric population. In addition to the excellent tolerance observed in patients, a significant increase over time in the PIMAX was demonstrated. Several studies have observed that atrophy of the diaphragm and other skeletal muscles in patients dependent on mechanical ventilation is quite common and occurs fast, starting within the first 24 hours of hospital admission [3,15-18]. Glau CL et al. [16] assessed 56 IMV dependent children using ultrasound and found that the diaphragm loses 3.4% of its thickness per IMV day, and that diaphragmatic atrophy is associated with increased IMV time and increased hospital stay.16 Despite the impact of diaphragmatic atrophy on late outcomes, studies discussing the functional rehabilitation of those patients are extremely rare. The patients included in our study presented complex diagnoses with multiple organ dysfunctions, with 9,000 hours of IMV time. Several authors have identified that specific risk factors such as prolonged mechanical ventilation [19-21], use of neuromuscular blockers [16], sepsis and multiple organ dysfunction syndrome [22-24] aggravated muscle mass loss. Most of these risk factors were identified in our population.
In our study, muscle atrophy was characterized by loss of muscle strength, which was assessed through PIMAX. Measurement of PIMAX is an effective method for assessing inspiratory muscles strength [25,26]. The maximum negative pressure generated during temporary airway occlusion is commonly used to measure inspiratory muscle strength in children under mechanical ventilation as it is easy to execute and is not invasive. A normal or almost normal rate of PIMAX is useful to rule out weakness of the respiratory muscles and obviates the need for complex and/or invasive testing [26-28]. So far, few pediatric studies have evaluated the effect of inspiratory muscle training on muscle strength and on clinical outcomes, such as the duration of ventilatory assistance [12-14], limiting themselves to the description of clinical cases. When considering a protocol for inspiratory muscle training, it was unclear whether moderate load training could cause muscle fatigue since the diaphragm contracts 24 hours/day without a break.
Our protocol was designed based on the recommended load for a peripheral muscle strength training program, in which it is established by physiology that 6 maximal or submaximal contractions produce an almost optimal increase in strength and no muscle fatigue. Our study has limitations. The first is the small number of patients in the sample. However, although our sample is small, we share how challenging it is to gather this number of patients and this study is the largest so far conducted with the pediatric population. The second is that the presence of complex diagnoses caused the stabilization of patients and the indication for IMT to occur after a long period of mechanical ventilation. The third is that there was no control group to compare strength gains in patients not submitted to the training protocol. Our study presented a safe and effective protocol for gaining PIMAX that favored the weaning of patients on prolonged mechanical ventilation, however, a randomized study and the presence of a control group is necessary for the validation of these findings.
Conclusion
Our study supports performance of IMT using moderate loads (60%) without risk of muscle fatigue, as it resulted in a significant increase in PIMAX after 2 weeks of training and in positive outcomes in weaning from mechanical ventilation. Finally, we suggest increase in PIMAX measurements for all children with prolonged use of IMT due to its low cost, applicability and to help clinicians to find the right time in the difficult decision of disconnecting these patients off the ventilator.
To Know more about Pediatrics & Neonatology
Click here: https://juniperpublishers.com/index.php



No comments:
Post a Comment